If you have spent any time online over the last couple of years, you have probably run into the growing conversation around psychedelic-assisted therapy. Psilocybin, the compound in “magic mushrooms,” is being studied at major universities, offered in supervised clinics in a handful of places around the world, and championed by doctors as a genuine breakthrough for depression, anxiety, and trauma.
That conversation is actually what prompted this article. I recently watched Dr. Tracy Kim Townsend, a licensed psilocybin facilitator and co-founder of Meadow Medicine, explain exactly how psilocybin therapy works in a YouTube video that you can find below:
It is a clear, straightforward explanation of the process, and I would recommend watching it if you want the psychedelic side of this story from someone who actually practices it. But watching it also crystallized a question I hear constantly from clients: can I get those same neurological breakthroughs without the chemical, the cost, or the legal complications?
The short answer is yes, more often than people expect. Hypnotherapy and psychedelic-assisted therapy look nothing alike on the surface, but they are aiming at the same neurological target. Both work by temporarily quieting the parts of the brain that keep us stuck in defensive, analytical loops, which opens a window for installing new automatic responses in their place. Understanding exactly how the two overlap, and exactly where they diverge, will help you make an informed choice about which path actually fits your situation. And since I want this to be a fair comparison rather than a sales pitch, I am going to include the research on psychedelic therapy’s downsides too, not just its upside.
I should say upfront that I am not writing this to dismiss psychedelic therapy or the people doing serious clinical work in that field. The research on psilocybin for treatment-resistant depression is real, and it deserves to be taken seriously. What I want to do here is lay out the actual neuroscience on both sides, including the parts of the psychedelic conversation that tend to get left out of the highlight reel, so you can see clearly why hypnotherapy achieves so much of the same result without the same trade-offs.
Quieting the Inner Narrator (Without the Risk)
Functional MRI research has shown that psilocybin temporarily quiets a brain network called the Default Mode Network, or DMN. Carhart-Harris and colleagues, in a landmark 2012 study published in the Proceedings of the National Academy of Sciences, found that psilocybin reduced coordinated activity within the DMN, and that this reduction correlated with what participants described as “ego dissolution,” a loosening of their normal sense of self.
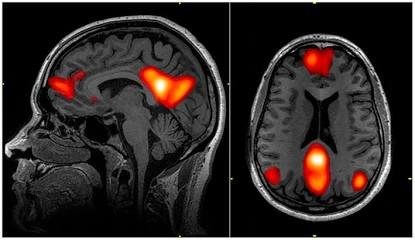
The DMN is essentially the part of your brain responsible for writing your internal autobiography. It is the seat of self-referential thought: the looping, rehearsed stories we tell ourselves about who we are, what happened to us, and what we are capable of. It is also the network most active when we ruminate on the past or spiral about the future. When the DMN goes quiet, the volume on that inner narrator drops, and other regions of the brain get a rare chance to talk to each other without the usual filter.
Here is the part that gets left out of most of the psychedelic conversation: hypnosis produces a strikingly similar effect, without any substance involved. In 2016, a team led by Dr. David Spiegel at Stanford University published fMRI research in the journal Cerebral Cortex showing that highly hypnotizable individuals, while under guided hypnosis, displayed decreased connectivity between the dorsolateral prefrontal cortex and the Default Mode Network. They also saw reduced activity in the dorsal anterior cingulate, a region involved in monitoring what deserves our attention and worry. Spiegel described the state plainly: when that region quiets down, “you’re so absorbed that you’re not worrying about anything else.”
That is the neurological signature of trance. It is not a metaphor and it is not a parlor trick. It is a measurable shift in how your brain’s attention and self-monitoring systems talk to each other, achieved through guided relaxation and focused language rather than a chemical.
It is worth pausing on why this matters outside of a research lab. The DMN is not just responsible for abstract self-reflection. It is running quietly in the background every time you catch yourself replaying an old argument, rehearsing a worst-case scenario before a work meeting, or automatically assuming the worst about a text that has not been answered yet. That constant narration is exhausting, and it is also largely automatic, which is exactly why willpower alone rarely dismantles it. Turning the volume down on that network, even briefly and safely, is what allows a new, calmer response to actually take hold instead of being shouted down by the old one.
The major practical difference is agency. During a psychedelic session, you hand control of your nervous system to a compound for several hours and have to ride out whatever comes up. During hypnosis, you remain fully conscious, alert, and in charge the entire time. You can open your eyes, speak, or stop the session whenever you choose. If you want to understand exactly what that state feels like from the inside and clear up the myths around it, I unpacked all of that in the truth about hypnosis, including why being hypnotized is closer to being deeply absorbed in a good book than being “under” anything.
Emotional Processing vs. Emotional Numbing
Traditional psychiatric medications, like most antidepressants, work by dampening emotional intensity. That can bring real relief, but it often leaves people feeling flattened or disconnected from their own lives.
Psychedelic-assisted therapy works in the opposite direction. It heightens emotional salience, meaning it increases the felt importance of whatever comes up during the session. By lowering psychological defenses, it can allow people to finally feel and release emotions they have been carrying, sometimes for decades.
Hypnotherapy operates on that same underlying principle of heightened emotional access, but with a meaningful difference in how the intensity is managed. Because hypnosis bypasses the analytical, defended part of the mind, it allows a client to safely access and metabolize stored emotional tension. The difference is that this happens incrementally. A skilled hypnotherapist paces the work so the nervous system can process a manageable amount at a time, rather than being flooded all at once. There is no risk of the kind of destabilizing, hours-long emotional flood that can happen in a psychedelic session, because the client’s conscious mind stays online and can signal when something needs to slow down.
This titrated pacing is not a lesser version of the psychedelic approach, it is a deliberate design choice. Think of the difference between opening a pressure valve gradually versus all at once. Both release the same pressure eventually, but one gives you control over the rate, and the other does not. For someone with a highly sensitized nervous system, or someone who has never done any kind of deep emotional work before, that control is not a minor convenience. It is often the difference between a session that feels productive and one that feels retraumatizing.
This matters most when the emotional material in question is old and load-bearing, meaning it is connected to how someone learned to feel safe, or unsafe, in the world. If you want to understand how the body and nervous system actually hold onto experiences like that long after the event itself has passed, I wrote a full breakdown in how the brain stores trauma, which explains why “just talking about it” so often is not enough on its own.
Activating Neuroplasticity to Change Habits
The real value of psilocybin, according to researchers studying it, is not just the experience itself but the window of heightened neuroplasticity that opens for several weeks afterward. Neuroplasticity is the brain’s capacity to reorganize itself and build new neural connections. That post-session window is when integration work has to happen: a deliberate stretch of time where the person has to actively practice new habits and new self-stories while the brain is unusually receptive to change.
Hypnotherapy does not just open a window of neuroplasticity and hope you use it later. It works inside that window in real time, during the session itself. EEG research on hypnosis has consistently found an increase in theta wave activity during trance, a frequency band closely associated with memory encoding and heightened learning capacity. That is not a coincidence. Neuroplastic change depends heavily on focused, emotionally significant attention, and that is precisely the state a well-guided hypnosis session creates: a deep, absorbed focus where distractions fall away and a specific suggestion becomes the primary content of consciousness.
By delivering targeted, positive suggestions while the brain is in that highly suggestible state, a hypnotherapist can help build and reinforce new neural pathways directly, in the chair, instead of waiting for an integration window to open after the fact. This is why hypnotherapy tends to be so effective for neutralizing compulsive, automatic patterns rather than just understanding them intellectually. There is also early clinical research actively measuring this in real time. A registered clinical trial currently underway in Istanbul is using EEG to track alpha, theta, and frontal asymmetry changes in patients with generalized anxiety disorder before and after a course of Ericksonian hypnotherapy, alongside standard anxiety measures like the Beck Anxiety Inventory. It is exactly the kind of study that will keep building the case for what hypnotherapists have observed clinically for years.
If you want a practical look at how this applies to breaking a specific unwanted pattern rather than just theory, I go deep on this in hypnotherapy for addiction, which walks through why targeting the root automatic response works better than relying on willpower alone.
The Risks Nobody Puts on the Brochure
I want to be fair to psychedelic-assisted therapy, because the research on its benefits for treatment-resistant depression and end-of-life anxiety is genuinely promising. But if we are being honest about the full picture, it comes with risks that hypnotherapy simply does not carry.
Post-acute side effects are more common than the optimistic framing usually suggests. A 2022 review by Breeksema and colleagues, along with separate research from Muller and colleagues the same year, documented flashback phenomena, lingering anxiety, panic symptoms, and depressed mood following psychedelic sessions, with severity varying case by case. A dose-response meta-analysis of psilocybin trials also found that the combined risk of prolonged psychosis and hallucinogen persisting perception disorder rises with dose. These events remain uncommon in supervised clinical settings, but they are not zero, and screening cannot catch every predisposition.
The psychiatric risk is not limited to rare edge cases either. A 2024 study by Simonsson, Mosing, Osika, and colleagues, published in JAMA Psychiatry, found an association between adolescent psychedelic use and the emergence of psychotic or manic symptoms. Other research has flagged elevated risk specifically in people with a personal or family history of psychotic or bipolar disorders, a population that is easy to miss without rigorous screening, and screening is exactly the kind of safeguard that gets skipped in unsupervised or recreational use.
Then there is the practical side, which matters just as much to most people weighing their options. In the United States, psilocybin remains a Schedule I controlled substance federally, meaning legal access is limited to a small number of state-regulated programs, clinical trials, or licensed facilitators in specific jurisdictions. In the United Kingdom, psilocybin is a Class A drug under the Misuse of Drugs Act, illegal outside of licensed research. Where legal supervised access does exist, sessions typically run into the thousands of dollars once preparation and integration support are factored in, and most insurance does not cover it.
It is also worth noting that most of the encouraging safety data on psilocybin comes from tightly controlled clinical trials with extensive pre-screening, a trained facilitator present for the entire multi-hour session, and a carefully prepared setting. That is a very different scenario from the general population actually accessing this treatment once it scales, and researchers studying real-world use have pointed out that rigorous trial screening tends to exclude exactly the people who would be most at risk for adverse outcomes in the first place.
Hypnotherapy carries none of that legal complexity or cost barrier, and it does not carry any risk of triggering psychosis, panic, or persisting perceptual disturbance, because there is no psychoactive substance altering your brain chemistry in the first place. You are simply guided into a naturally occurring, well-researched state of focused attention that your brain already knows how to enter.
Bypassing the Ego to Heal Early Conditioning
When the Default Mode Network quiets down, whether through psilocybin or through hypnosis, we get access to deeper, younger parts of the psyche that hold our earliest conditioning. This is where a lot of our core beliefs about safety, worthiness, and connection were originally written, usually long before we had the language to question them.
Psychedelics can bring this material forward in sudden, intense rushes of insight, which is part of why integration support afterward is considered essential rather than optional. Hypnotherapy takes a more structured, conversational route to the same layer. By engaging in targeted inner child work while the client is deeply relaxed and the analytical defenses are quieted, we can pinpoint the specific moments where a limiting belief was formed, and update it while the nervous system is receptive.
This kind of gentle regression tends to resolve relationship patterns that logic alone rarely touches, because those patterns were never installed logically in the first place. If this is a piece of your own story, I walk through the full process in how to heal childhood wounds, including how codependent patterns trace back to this exact layer of conditioning.
So Which Path Actually Fits You?
Neither modality is universally “better.” They are built for different circumstances, and being honest about that is more useful than picking a side.
Psychedelic-assisted therapy, under proper clinical supervision, has shown real promise for treatment-resistant depression and end-of-life distress in patients who have not responded to other approaches and who have been carefully screened for risk factors like a personal or family history of psychosis. It is a legitimate medical intervention, but it is also a bigger swing: more intense, less controllable in the moment, and currently harder to access.
Hypnotherapy tends to be the better starting point for the vast majority of people dealing with anxiety, phobias, compulsive habits, low-grade trauma responses, and the kind of early conditioning that keeps showing up in adult relationships and self-talk. It is repeatable, affordable, does not require a medical screening process to rule out psychiatric risk factors, and puts you in the driver’s seat of your own healing from the first session. For a lot of people, it is not a consolation prize next to psychedelic therapy. It is the more sustainable long-term tool, and one you can return to as often as you need without cost or legal barriers standing in the way.
Head-to-Head: Comparing the Two Paths
| Psychedelic-Assisted Therapy | Guided Hypnotherapy |
| Quiets the Default Mode Network chemically, through serotonin receptor activity | Quiets the Default Mode Network naturally, through guided attention and relaxation |
| Requires surrendering control to a chemical process that cannot be paused once it begins | Fully conscious, alert, and able to stop or redirect the session at any point |
| Intense, sudden catharsis that can feel overwhelming even with support present | Controlled, titrated emotional release paced to what your nervous system can handle |
| Documented risk of post-acute anxiety, flashbacks, and rare prolonged psychiatric symptoms | No risk of triggering psychosis or persisting perceptual disturbance |
| Legally restricted in most places; typically thousands of dollars per session | Legal, accessible, and dramatically more affordable, with no clinical screening required |
| Requires weeks of dedicated post-session effort to lock in change | Builds new neural pathways in real time, during the session itself |
Where to Go From Here
If any of this resonated, whether it is the anxiety, the compulsive patterns, or the early conditioning that keeps quietly running the show in your relationships, that is exactly the kind of work I do one on one. You do not need a clinical referral, a legal gray area, or a multi-thousand-dollar retreat to start rewiring these patterns. You need a guided process your brain already knows how to enter.
You can book a call directly at markstubbles.com/book-a-call and we will figure out together what the most direct path looks like for what you are carrying.






Leave a Reply