You might tell yourself it’s just nerves. A flicker of heat rising in your cheeks before a presentation, after a mistake, or when someone looks at you a beat too long. You might have spent years hoping people wouldn’t notice, changing your behaviour to avoid triggers, or feeling quietly ashamed of a reaction you cannot seem to control.
Most people, even many therapists don’t fully appreciate: blushing is not a personality flaw. It is not shyness dressed up in physiological clothing. In many cases, chronic, involuntary blushing is the body’s language for something it has never been given the chance to say out loud.
Trauma isn’t only stored as memories, flashbacks, or intrusive thoughts. It is stored in the body, in the tissues, nerves, and reflexes that govern how you move through the world. When the nervous system has been conditioned by threat, it will find ways to signal danger even when no danger exists. Blushing, for many people, is exactly that signal.
| “The body keeps the score.” — Dr. Bessel van der Kolk, psychiatrist and trauma researcher. This phrase captures something clinically essential: the residue of overwhelming experience is held not just in the mind, but in the automatic, sub-cognitive responses of the body itself. |
In this post, we will explore the neuroscience behind why trauma causes involuntary physical responses like chronic blushing, how a condition known as erythrophobia fits into the broader picture of somatic trauma, why traditional talk therapy often falls short, and how hypnotherapy offers a route to genuinely resetting the nervous system’s threat response.
The Science of the Survival Loop
The Amygdala: Your Brain’s Alarm System
At the centre of all threat-based responding sits a small, almond-shaped structure deep in the brain: the amygdala. Its job is elegantly simple, scan the environment for danger and trigger a response before the thinking brain has time to catch up.
In an acute crisis, this is a life-saving feature. When you pull your hand away from a hot stove before you’ve consciously registered ‘pain,’ that’s your amygdala at work. It is fast, automatic, and profoundly good at keeping you alive.
The problem arises when the amygdala has been recalibrated by trauma. After a prolonged period of stress, abuse, humiliation, or any experience that overwhelmed the nervous system’s capacity to cope, the amygdala can become chronically sensitised. It starts to read neutral, even safe situations as threats. It fires the alarm not because danger is present, but because the pattern resembles something that was once dangerous.
| Think of it like a smoke detector that has been set too sensitively after a kitchen fire. Long after the fire is out, the smell of toast sets it off. The alarm is real. The response is real. But the threat level has been misread. |
From Parasympathetic to Sympathetic: The Autonomic Shift
The autonomic nervous system (ANS) operates in two primary modes. The parasympathetic branch governs rest, digestion, connection, and recovery. What we colloquially call the “rest and digest” state. The sympathetic branch governs emergency responses: the surge of adrenaline and cortisol, the acceleration of heart rate, the diversion of blood to the muscles, and the heightened state of alertness we know as fight-or-flight.
In a healthy, regulated nervous system, these two branches work in balance, shifting fluidly between activation and recovery depending on what the environment demands.
In a trauma-conditioned nervous system, this balance is disrupted. The sympathetic branch becomes dominant, triggering the physiological hallmarks of threat response including dilation of superficial blood vessels even when the perceived threat is a social one, such as being observed, judged, or put on the spot.
Blushing, at its most fundamental level, is a sympathetic nervous system event. It is caused by the rapid vasodilation of blood vessels in the face, neck, and chest in response to perceived social evaluation. In people with a trauma-sensitised nervous system, this response is not just occasional. It is a hair trigger, set to fire at the slightest social signal of scrutiny.
The Survival Loop: When the Alarm Never Switches Off
One of the most important concepts in somatic trauma work is what we might call the “survival loop” — a self-perpetuating cycle in which:
- A social or emotional trigger activates the sympathetic nervous system
- The body responds with physical symptoms (blushing, sweating, shaking, heart racing)
- The person notices the physical response and becomes anxious about it
- That anxiety itself becomes a new trigger, intensifying the sympathetic activation
- The cycle repeats, reinforcing the neural pathway with every iteration
Over time, this loop becomes encoded in the body as a default pattern. The nervous system doesn’t distinguish between ‘I am in danger’ and ‘I might be seen to blush,’ both fire the same cascade of physiological responses. The body has learned to treat social vulnerability as a survival threat.
Erythrophobia as a Trauma Response
Defining Erythrophobia
Erythrophobia — from the Greek erythros (red) and phobos (fear) — is defined as a persistent, intense fear of blushing. It is recognised within the broader category of social anxiety disorder, but it warrants specific attention because it involves a particularly cruel double-bind: the fear of blushing is itself one of the most reliable triggers for blushing.
But describing erythrophobia simply as ‘shyness’ or ‘social anxiety’ undersells its complexity and its roots. For many sufferers, erythrophobia is better understood as a specific somatic manifestation of hypervigilance. The body’s learned state of chronic readiness for threat.
Hypervigilance is a hallmark symptom of trauma. It describes a nervous system that has been calibrated to scan constantly for danger, to interpret ambiguous signals as threatening, and to mobilise the survival response before conscious thought can intervene. In erythrophobia, that hypervigilance is focused specifically on the social domain. The threat of being seen, evaluated, and found wanting.
| Erythrophobia is not vanity. It is not oversensitivity. For many sufferers, it is the surface expression of a nervous system that learned, in conditions of threat or shame, that being visible is dangerous. |
What the Research Tells Us
Drummond et al. (1997, 2003): The Prolonged Physiological Response
One of the landmark findings in erythrophobia research comes from the work of P.D. Drummond and colleagues, whose studies across the late 1990s and early 2000s demonstrated something clinically significant: people with a fear of blushing do not just blush more frequently, their nervous systems take measurably longer to return to baseline after a blushing episode.
In other words, the physiological arousal stays ‘heated’ for longer. This is not a matter of being overly dramatic or hypersensitive in a psychological sense, it is a measurable difference in autonomic recovery time. The nervous system of someone with erythrophobia has learned to stay on alert even after the triggering event has passed, as though it does not trust the threat to be truly over.
This prolonged recovery is consistent with what we see in trauma-conditioned nervous systems more broadly: a reduced capacity for the parasympathetic ‘rest and recover’ response to reassert itself after sympathetic activation.
Nikolić et al. (2015): Blushing as a Physiological Marker of Social Threat Detection
A meta-analysis by Nikolić and colleagues published in 2015 provided important confirmation that blushing is not simply an emotional response, but a reliable physiological marker of what they described as social anxiety and trauma-based threat detection.
The research highlighted the degree to which blushing functions as an involuntary signal, one that the individual experiencing it has little conscious control over, and underscored the relationship between chronic blushing and the kind of hyperactivated threat-detection systems seen in anxiety disorders with traumatic origins.
This is important for two reasons. First, it validates the experience of erythrophobia sufferers who often describe feeling entirely at the mercy of their blush. Second, it points toward the need for interventions that address the threat-detection system at a neurological level, rather than simply reframing thoughts at a cognitive level.
Laederach-Hofmann et al. (2002): Abnormal Autonomic Regulation Under Stress
Research by Laederach-Hofmann and colleagues added another dimension to the clinical picture by demonstrating that patients with erythrophobia exhibit what the authors described as ‘abnormal autonomic regulation’ under conditions of mental stress.
The autonomic nervous system, in these individuals, responds to mental and emotional stressors in ways that are dysregulated, that is, the normal feedback mechanisms that would otherwise moderate the stress response appear to be functioning differently. This aligns with the broader literature on autonomic dysregulation in trauma, and points toward the profound physiological nature of the condition.
Taken together, these three bodies of research paint a compelling picture: erythrophobia is not a quirk of personality or a product of excessive self-consciousness. It is a condition with measurable physiological underpinnings, rooted in the same kind of nervous system dysregulation that characterises traumatic stress responses.
Why Traditional ‘Talk’ Therapy Often Falls Short
The Old Brain vs. the New Brain
To understand why cognitive and verbal therapies: CBT, counselling, psychodynamic therapy often produce limited results for erythrophobia and somatic trauma responses, we need to understand a fundamental architectural feature of the human brain.
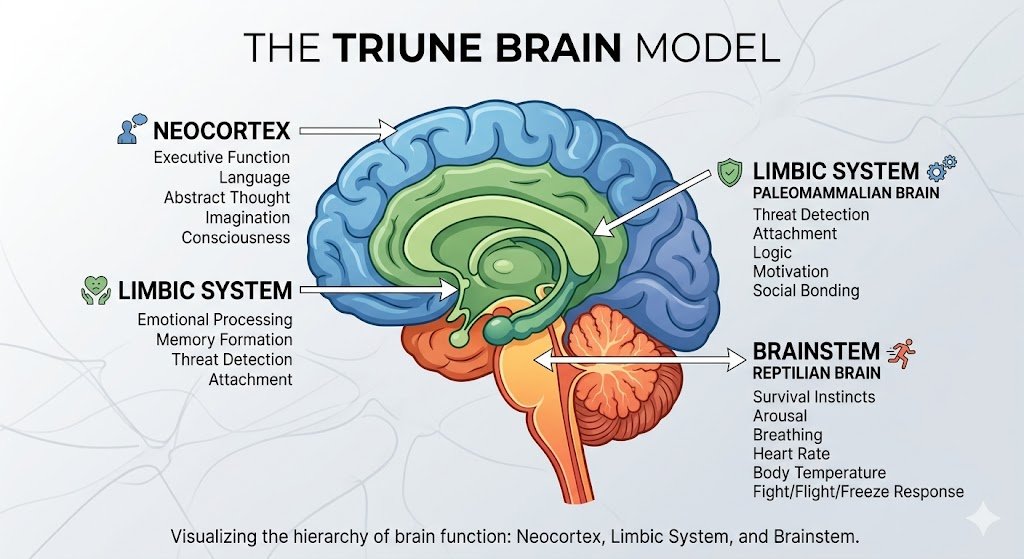
The brain can be loosely understood in terms of three functional layers, sometimes described as the ‘triune brain’:
- The neocortex (prefrontal cortex): responsible for rational thought, language, planning, and conscious reflection — the ‘new brain’
- The limbic system: the emotional brain, responsible for memory, attachment, and emotional processing — including the amygdala
- The brainstem and cerebellum: responsible for automatic, survival-oriented functions — the ‘old brain’
Talk therapy works primarily in the realm of the prefrontal cortex. It engages language, narrative, insight, and conscious reflection. For conditions that are primarily cortical; patterns of thinking, for example, or distorted beliefs this is exactly the right tool.
But blushing is not a cortical event. It is generated by the brainstem and limbic system, structures that predate language, that do not ‘think’ in any conventional sense, and that are not directly accessible through conversation. You cannot talk your amygdala out of its threat response any more than you can consciously slow your heart rate by reasoning with it.
| “Trauma is not stored in the narrative memory. It is stored in the body, in sensation, in the reflexes that fire before thought can intervene. Healing it requires working below the level of language.” — Mark Stubbles, Hypnotherapist & Trauma Specialist |
The Limits of Cognitive Reframing
Many erythrophobia sufferers have spent years in therapy, have done the cognitive reframing exercises, understand intellectually that blushing is harmless, that others probably don’t notice as much as they think, that their worth is not conditional on never flushing red.
They know all of this. And they still blush.
This is not a failure of intelligence or commitment. It is evidence that the problem exists at a level below cognitive access. When the survival system is activated, the prefrontal cortex goes partially offline, a process researchers call ‘cortical inhibition.’ In other words, the very brain regions that talk therapy targets become less available precisely when they are most needed.
This is why people often describe knowing rationally that they are safe while simultaneously feeling physically, viscerally that they are in danger. Both are true, in their own way, for their own brain region. The challenge is bridging the gap between them.
Healing the Physical Response: The Role of Hypnotherapy to Stop Blushing
Communicating Below the Level of Thought
Hypnotherapy is not stage magic. It is not about being ‘under someone’s control’ or surrendering your will. In a clinical context, hypnotherapy is a powerful method for inducing a profoundly relaxed, focused state of awareness. A state in which the critical, analytical filters of the prefrontal cortex are gently set aside, creating direct access to the limbic system and the autonomic nervous system.
This is precisely the access that makes hypnotherapy uniquely suited to working with conditions like erythrophobia and somatic trauma responses. Where talk therapy knocks on the front door of the conscious mind, hypnotherapy finds a window directly into the old brain. The part of the nervous system where the threat response lives, where the survival loop runs, where the physiological conditioning was laid down.
Why Hypnotherapy for Blushing is Effective
In the context of treating erythrophobia, hypnotherapy works through several interconnected mechanisms:
1. Nervous System Recalibration
The deep relaxation achieved in a hypnotic state is itself a powerful activator of the parasympathetic nervous system. By guiding the client into a state of profound physiological calm repeatedly and consistently, the nervous system begins to build new associations. Social situations, which have long been paired with sympathetic activation, can begin to be paired instead with safety, ease, and calm.
2. Accessing and Reprocessing the Root Cause
Hypnotherapy allows a trained practitioner to help clients access the earlier experiences, often rooted in childhood or adolescence that initially calibrated the nervous system to treat social visibility as a threat. By revisiting these experiences in a state of safety, the emotional charge can be reduced, and the neural associations can begin to shift.
3. Installing New Physiological Responses
Using suggestion, visualisation, and somatic techniques within the hypnotic state, the practitioner can help the client begin to rehearse new responses at a neurological level. The nervous system does not fully distinguish between a vividly imagined experience and a real one, this is the foundation of mental rehearsal used by elite athletes, surgeons, and performers. The same principle applies to rehearsing calm, confident responses to previously triggering social situations.
4. Reducing the Anticipatory Anxiety Loop
Because so much of erythrophobia’s power lies in the anticipation, the dread of blushing that itself triggers blushing hypnotherapy’s ability to interrupt this loop at an unconscious level is particularly valuable. By addressing the anticipatory fear directly, in the very state where it originates, the self-perpetuating cycle can be broken. In this post I spoke about my own experience of erythrophobia and anticipatory anxiety.
| Hypnotherapy does not suppress the blush through force of will. It addresses the underlying miscalibration of the nervous system. The alarm stops firing where there is no fire. |
What the Process Actually Looks Like
Working with a hypnotherapist specialising in erythrophobia and somatic trauma involves an initial thorough consultation to understand your specific history, triggers, and goals. Sessions typically involve guided relaxation, specific language patterns designed to communicate with the autonomic nervous system, and carefully tailored suggestion work that is built around your individual case rather than a generic script.
The work is collaborative, gentle, and entirely within your control. Many clients report noticing shifts both in their physiological responses and in their relationship with the prospect of blushing. These shifts occur within a relatively small number of sessions, though meaningful and lasting change typically unfolds over time.
Why Online Hypnotherapy Works Particularly Well for Blushing
One practical advantage that is worth naming directly: for people dealing with blushing and social anxiety, online hypnotherapy removes one of the biggest barriers to getting help in the first place.
Having to travel to a therapist’s office, sit in a waiting room, and interact with reception staff is, for many erythrophobia sufferers, already a gauntlet. The anticipation of being observed, evaluated, or seen to flush before the session has even begun can be enough to put people off entirely.
Working via an encrypted video call such as Zoom means you can have your session from wherever you feel most at ease, your own home, your bedroom, a quiet room you trust. That familiarity matters. When the nervous system is not already primed by the journey and the waiting, the depth of relaxation available in session is often greater, and the work can move more quickly as a result.
Anxious people also tend to make excellent hypnotic subjects. The same imagination that replays worst-case scenarios and catastrophises about future situations is, when redirected, a powerful tool for change. Hypnosis does not require you to switch off your anxiety. It works with the mind you already have and begins, gradually, to show it something different.
Complementary Tools: What to Use Between Sessions
Hypnotherapy works on the underlying pattern, but it is also useful to have practical tools you can reach for in the moment, or in the days between sessions. Two approaches stand out for being discreet, effective, and genuinely calming to the nervous system.
EFT (Emotional Freedom Technique)
EFT, sometimes called tapping, involves applying gentle pressure to specific acupressure points on the body while focusing on the sensation you want to shift. In a social situation, this can be done discreetly, for example by pressing a fingertip to a point on the side of your hand or beneath your collarbone, while bringing your attention to the physical feeling of that contact rather than the anxiety in your face.
The technique works by giving the nervous system a competing sensory input, something concrete and present to focus on, which interrupts the internal monitoring loop that feeds blushing. It does not cure erythrophobia, but used consistently alongside hypnotherapy, it can take the edge off an acute episode and help you stay grounded in the moment rather than spiralling into anticipatory dread.
Breathing Techniques
Breathing is one of the only autonomic functions we can consciously control, and that makes it a direct lever on the nervous system. Two patterns are particularly useful for blushing.
Box breathing involves inhaling for a count of four, holding for four, exhaling for four, and holding again for four before the next breath. The regularity of the pattern is itself calming, pulling the mind out of catastrophic thinking and into a simple, repeatable sequence.
Seven-eleven breathing is even more targeted: inhale for a count of seven, exhale for a count of eleven. The extended exhale is key. If you were genuinely in a life-or-death situation, the last thing your body would do is produce a long, slow out-breath. By doing exactly that, you send the nervous system a signal that contradicts the threat response: there is no emergency here. The body tends to believe it.
Both techniques are available as free recordings on Mark’s YouTube channel, alongside a free hypnosis session specifically for blushing, if you want to hear them guided before trying them on your own.
These tools work best as a bridge. They manage the surface symptom in the moment while hypnotherapy works on the deeper pattern that is causing it.
Moving Forward: A Different Relationship with Your Body
If you have lived with chronic blushing or erythrophobia, you may have come to see your body as the enemy, a source of embarrassment and betrayal, something that reveals you at the worst possible moments. The framing this post offers is a different one.
Your nervous system learned what it learned in conditions that were, at the time, genuinely overwhelming. The survival loop it built was a reasonable, even intelligent response to an environment that felt threatening. It is not a character flaw. It is not evidence that something is fundamentally broken about you.
But it is also not something you have to keep living with.
The neuroscience is clear: nervous systems that have been conditioned by experience can be reconditioned by new experience. The brain remains plastic, capable of building new associations, new pathways, new defaults throughout life. The survival loop that has run on autopilot for years can be interrupted, rewired, and ultimately replaced with something that serves you better.
That process takes the right kind of support. Not support that tries to reason with a system below the level of reason, but support that meets the nervous system where it actually lives and helps it learn, at last, that the threat is over.
| Ready to work directly with your nervous system?Explore the Beyond Blushing E-book — a deep-dive resource designed to help you understand and begin to resolve chronic blushing from the inside out. markstubbles.com/product/beyond-blushing-e-book Or explore one-to-one Hypnotherapy for Blushing sessions: markstubbles.com/hypnotherapy-to-stop-blushing |
References & Further Reading
Drummond, P. D. (1997). The effect of adrenergic blockade on blushing and facial flushing. Psychophysiology, 34(2), 163–168.
Drummond, P. D. (2003). Blushing inhibited by oxprenolol in social phobia: A pilot study. Journal of Anxiety Disorders, 17(1), 37–44.
Nikolić, M., Colonnesi, C., de Vente, W., Drummond, P., & Bögels, S. M. (2015). Blushing and social anxiety: A meta-analysis. Clinical Psychology Review, 40, 14–27.
Laederach-Hofmann, K., Mussgay, L., Büttner, M., Klinkenberg, N., & Rüddel, H. (2002). Patients with erythrophobia (fear of blushing) show abnormal autonomic regulation in mental stress conditions. Psychosomatic Medicine, 64(2), 358–365.
van der Kolk, B. A. (2014). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Viking.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton & Company.






Leave a Reply